
Reykjavik 26th of July 2017
Cutaneous silent period can be
preserved in entrapment neuropathies (KofIer et al 2003).
It is known that the more severe the neuropathy is, the more impairment of
A-delta fibers can be found (Duarte et al 2016).
In patient with severe CTS the mean onset latency was increased to 85.0 ms
(SD 8.7 ms, P < 0.01) Silvpauskaite
et al 2005.
CASE
REPORT (here) Patient 66 year-old with motor weakness in hands and
hypoesthesia
This case was published in Neurophysiology Plus Iceland informal group e-Bulletin (here)

Right median nerve mixed and cutaneous (palm) silent period

Cutaneous Silent Period from 2 digit sensory branches (ring electrodes)
Cutaneous Silent Period from 2 digit sensory branches in examinator (OCB), normal values
After we diagnosed very severe
CTS in the right side and severe CTS in the left we performed A-delta & alpha
motorneurons driven CSP from 2 digit and there was no clear inhibition of the
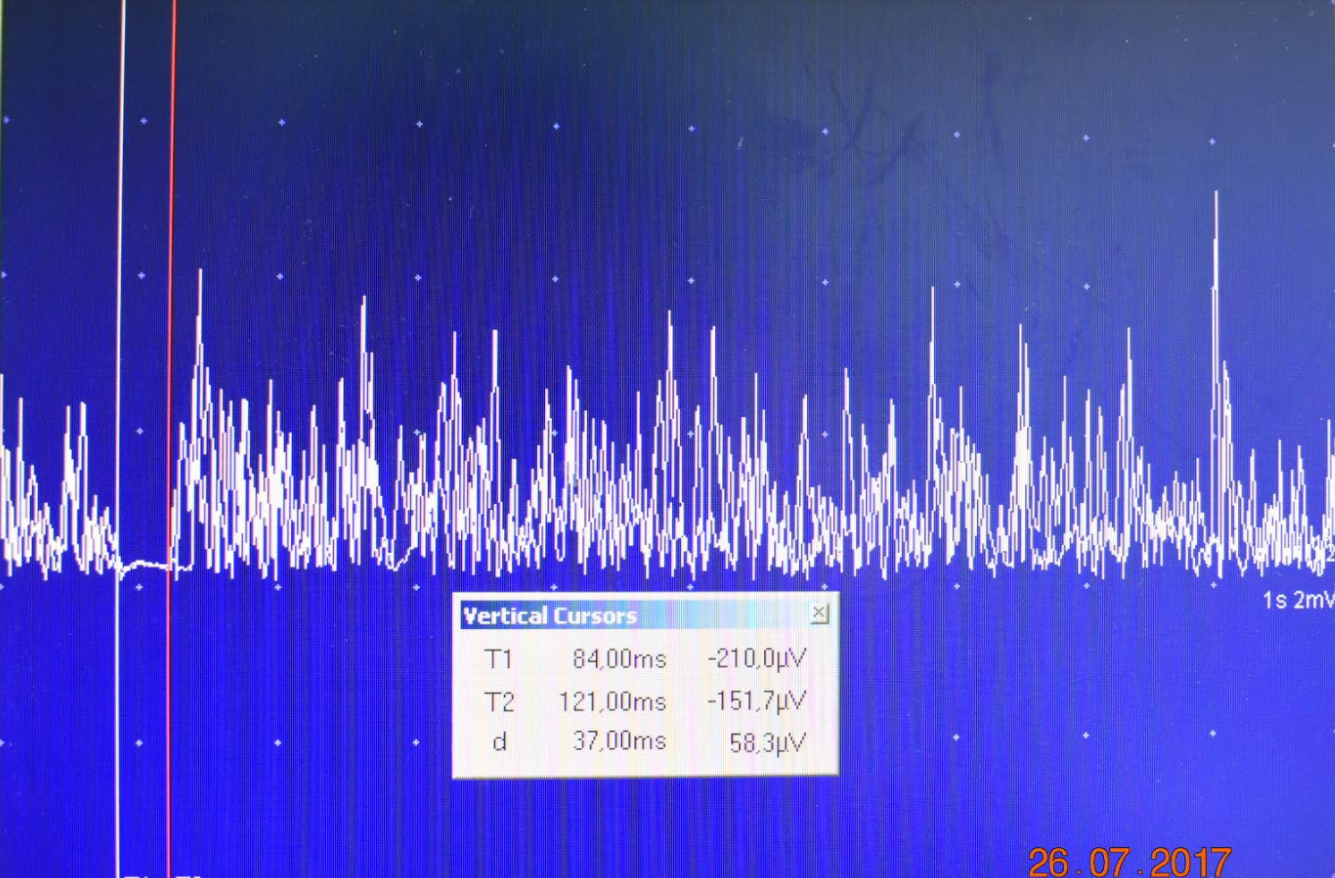
voluntary contraction (onset 107ms). Then, we checked again from the
palm-thenar region and we observed CSP with onset 100ms, end 155 ms and 55ms
duration. Also a clear silent period was obtained after stimulation from the
wrist, the mixed median nerve and record from abductor pollicis brevis.
Conclusion: Sensory fibers (small and fast) are
the last in be damaged and the injury do not occurred at the wrist carpal
tunnel as it happened with axonal loss of the large sensory fibers. At this moment there is not clear if those
fibers are only the A-delta or there might be another sensory input by direct
electrical stimulation of other fiber type (proprioceptors?, muscle spindles?)

Nerve Conduction Studies: 2017 © Neurophysiology Plus Iceland












